
Hip Dips: How to get rid of them...
- Skye Sunderland

- Apr 24
- 5 min read
“Let’s fix your hip dips…”
Actually, I only said that to get you here...
Now that you are here, I’m going to tell you something most fitness influencers will never say clearly enough.
You’ve been misinformed about what hip dips actually are.
And once you understand anatomy, the idea of “fixing” hip dips stops making sense.
What hip dips actually are
Hip dips are not a flaw, imbalance, or missing muscle. They are a visible expression of how your skeleton is shaped, and how soft tissue sits on top of it.
More specifically, they reflect the relationship between three things:
Pelvic bone structure
Femoral bone positioning
Distribution of muscle and fascia over those structures
At the centre of this are two key anatomical landmarks:
The iliac crest (the top rim of your pelvis)
The greater trochanter (a bony prominence on the femur)
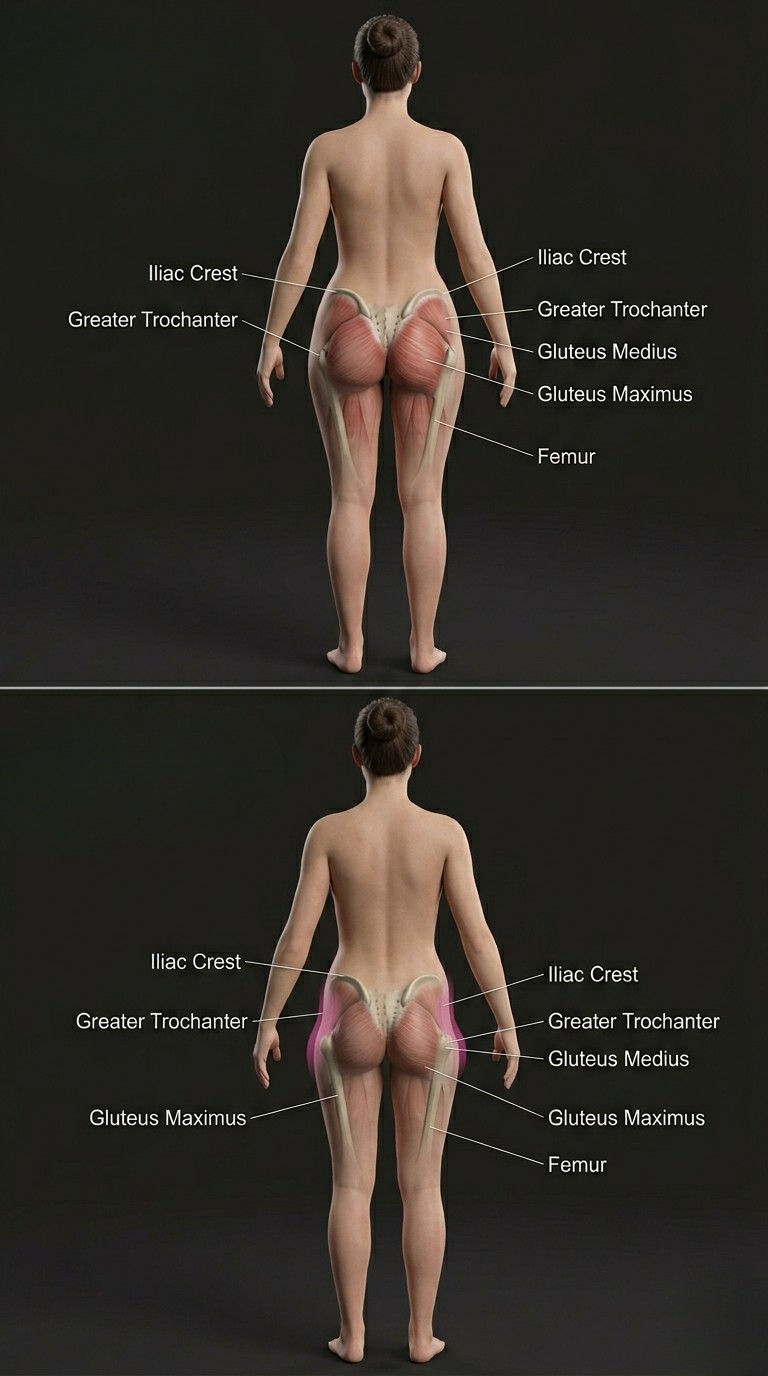
Everything you see on the outer hip exists between these two fixed points.
That space is what creates variation in hip shape across humans.
The pelvis: why structure changes shape
To understand hip dips properly, you have to start with the pelvis. The pelvis is not a flat structure. It is a complex, three-dimensional ring designed for load transfer, movement efficiency, and in females, reproductive function.
There is a well-documented pattern of sexual dimorphism in pelvic structure:
Females tend to have a wider pelvic inlet
Greater lateral flare of the iliac crest
A shorter vertical pelvic height relative to femur length
Increased transverse pelvic width

On average, the iliac crest in females is approximately 5–10° more laterally flared compared to males. This is not a dramatic difference, but in biomechanics, small angular differences create large visual changes over distance.
However, this is where most explanations go wrong:
These are average trends, not rules.
There is large individual variation in pelvic morphology across all sexes. Two women can have completely different pelvic shapes. Two men can as well.
This variation is one of the primary reasons hip dips are not universal.
They are not a “female trait.”
They are a structural trait that appears differently depending on bone geometry.
The hip joint: where the system connects
The hip joint sits deep within the pelvis at the acetabulum, which is the socket that receives the head of the femur. This is a true ball-and-socket joint, designed for both stability and mobility.
The orientation of the acetabulum influences how force is transmitted through the femur during movement such as walking, squatting, and running.
From a structural perspective, the acetabulum acts as the central load-bearing interface between pelvis and femur.
Femoral positioning and anteversion
The femur is not a straight, fixed rod sitting under the pelvis. It has rotational variability. One of the most important variables is femoral anteversion, which refers to the inward rotation of the femoral neck relative to the distal femur. In adults, this typically falls within a range of 10–20 degrees, although there is significant individual variation.
This angle affects:
How the femur sits inside the acetabulum
The direction the thigh projects from the pelvis
The spatial relationship between the pelvis and lateral femur
Even small differences in femoral rotation change how the outer hip contour appears, because they shift where the femur sits relative to the iliac crest.
This is one reason hip shape can look different even between people with similar training status.
The key structural relationship
Now we bring it together. The outer hip contour is defined primarily by the distance and angle between:
The iliac crest (top of pelvis)
The greater trochanter (outer femur)
These are fixed anatomical landmarks.
They do not change with exercise.
They do not change with glute activation.
They do not change with hypertrophy.
What changes is the soft tissue that sits over them.
But the underlying spacing remains the same.
This is critical.
Because hip dips are not a “gap in muscle.”
They are a transition in bone structure.
Muscle anatomy of the lateral hip
The hip is covered by multiple muscle groups that sit in different planes and perform different functions.
Gluteus medius
Origin: lateral surface of the ilium
Insertion: lateral surface of the greater trochanter
Function: pelvic stabilisation during single-leg stance
This is one of the most important muscles for gait efficiency and frontal plane control.
Gluteus minimus
Origin: external surface of the ilium (deep to medius)
Insertion: anterior aspect of the greater trochanter
Function: hip stabilisation and internal rotation control
This muscle works synergistically with glute med in stabilising pelvic drop during movement.
Gluteus maximus
Origin: posterior ilium, sacrum, coccyx
Insertion: femur and iliotibial band
Function: hip extension and force production
This is the largest and most superficial gluteal muscle.
It contributes significantly to posterior hip volume, but it sits more posteriorly than laterally.
Tensor fasciae latae (TFL)
Origin: anterior iliac crest
Insertion: iliotibial band
Function: fascial tensioning and hip stabilisation
This muscle blends into the IT band, which runs down the lateral thigh.
Why muscle doesn’t “fill” hip dips
Here is the key misunderstanding. Muscles do not create a continuous, uniform surface over the hip. They attach at specific points. They follow directional lines of force. And they sit over a three-dimensional bony structure that has fixed geometry.
Between the iliac crest and greater trochanter, there is a natural transition zone where:
Bone shape changes direction
Muscle thickness varies by region
Fascia spans across tension lines
This means soft tissue is not evenly distributed across the lateral hip.
So, depending on the underlying skeletal structure, that transition can appear:
Smooth
Slightly indented
More visibly curved inward
None of these outcomes indicate dysfunction.
They are structural variations.
Why hip dips are more or less visible
Hip dip visibility is influenced by three main factors:
1. Pelvic width and shape
A wider pelvis increases the lateral distance between iliac crest and femur, which can make the transition zone more noticeable.
2. Femoral angle (anteversion)
Changes how the femur sits under the pelvis, altering external hip projection.
3. Soft tissue distribution
Muscle thickness, fascial tension, and fat distribution all influence surface contour.
Importantly, none of these factors are purely “trainable in isolation.”
They are structural or systemic variables.
What training actually does (and doesn’t do)
This is where confusion is most common. Training absolutely matters for the glutes.
Resistance training can:
Increase gluteus maximus hypertrophy
Improve gluteus medius strength and stability
Enhance pelvic control and movement efficiency
Improve force transfer through the hip joint
But training cannot:
Change pelvic width
Alter femoral bone structure
Modify acetabular orientation
Eliminate the transition between bony landmarks
So, while glute training improves shape, strength, and performance, it does not erase structural anatomy. In some cases, increased muscle mass can even make the transition more visible, simply by increasing contrast between regions. This is not a negative outcome. It is a predictable anatomical one.
So what are hip dips actually?
Hip dips are simply:
A normal variation in how skeletal structure and soft tissue interact along the lateral hip.
They reflect:
Bone geometry
Joint orientation
Muscle insertion points
Individual tissue distribution
They are not a defect.
They are not a weakness.
They are not a “problem area.”
They are part of normal human variation.
Why the “fix your hip dips” narrative is misleading
The idea that hip dips can be “fixed” implies that:
They are caused by muscle deficiency
They are reversible through targeted exercise
There is an optimal hip shape everyone should achieve
Anatomically, none of these are accurate.
What is actually happening in most of this content is a mismatch between:
Structural anatomy
And aesthetic marketing
Exercises can improve function and muscle size.
They cannot rewrite skeletal geometry.
A strong hip is not defined by a smooth lateral contour.
It is defined by:
Stability under load
Force production
Control through range of motion
Efficient movement mechanics
Hip dips do not reduce performance.
They do not indicate weakness.
They do not need correction.
They are simply one of many ways the human hip can be structured.
The issue was never your body.
It was the explanation.

Comments